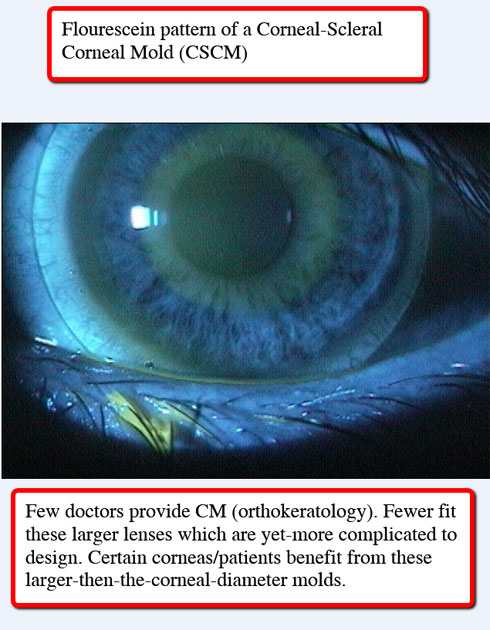
Corneal Molding (CM) is better known as Orthokeratology. It is a process of sleeping with specially designed corneal molds (fancy rigid gas permeable contact lenses) which change the curvature of the cornea. After waking, when the patient removes the lens they can see great all day WITH NOTHING IN THEIR EYES.
It can be enjoyed by people of all ages and those who have nearsightedness (myopia), farsightedness (hyperopia), astigmatism and the need for bifocals (presbyopia). A huge added benefit for the younger patient who suffers from continuing worsening of their vision (stronger glasses every year…) is this molding process stops, to significantly slows that progression. This, by itself, answers one of the greatest requests by parents: “How can I keep my child’s eyes from getting worse every year?”
Dr. Wilcox likes to simplify things and uses a lot of analogies. He has concluded that there are 4 reasons why people don’t or should not pursue corneal molding.
“Because I say so.” Simply put, Dr. Wilcox will not direct anyone toward any procedure or choice which is not appropriate for that person, PERIOD. This principle applies to everything he does and offers.
Cost. Corneal molding has greater costs than traditional glasses or soft contact lenses but, those options do NOT offer what CM provides. The fees are tiered because not all patients are the same. Some prescriptions are more complicated than others, some corneas are more challenging to mold. Some CM goals will need more expensive materials. Some people have more complicated vision needs and so on… Once we evaluate the patient we can then present the appropriate fees for that case. CM is rarely practiced by other eye doctors because it is not easy to do, because it takes a great deal of expertise, because it takes a passion and commitment to perform correctly and because Dr. Wilcox is a respected world leader in CM. He is frequently published in the Optometric literature, he lectures to National and International audiences on this and other topics. Dr Wilcox is a consultant to various contact lens manufacturers.
Chicken! Simply put, that applies to the patient who is afraid to touch their eyes. This is RARELY a barrier. At times some children are not ready to touch their eyes OR be responsible enough to insert the molds on a nightly basis. Though the youngest patient Dr. Wilcox has molded was 6 years old, there are some 12 year olds who are not mature or confident enough to mold. A little time and education can amend that impasse.
Unreal Expectations You have to mold every night (OK, some patients with lower prescriptions can skip nights but that is the exception and not the rule). CM is not for firemen who have unpredictable sleep hours. It will not ‘fix a blind eye’. It is not proper for all prescriptions. All of this is linked to #1 as well.
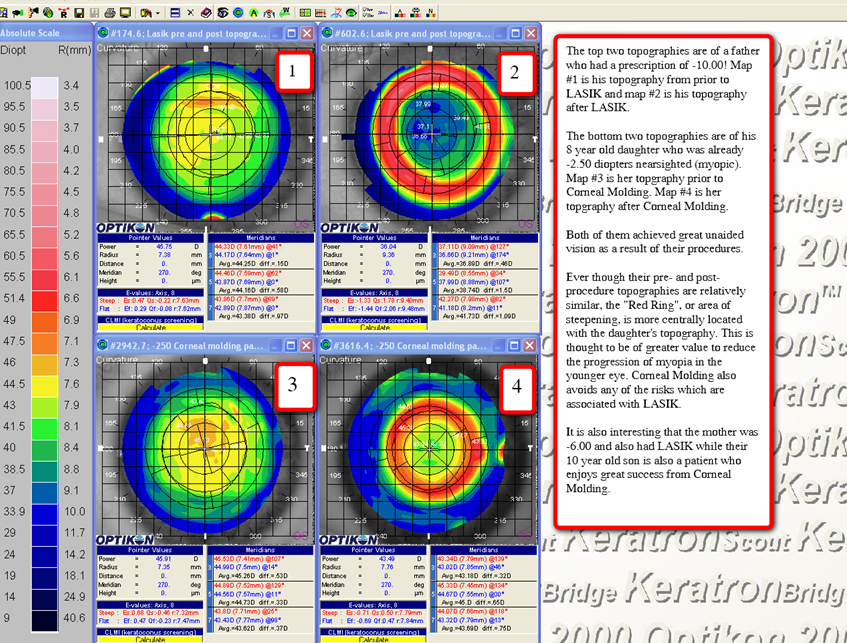
CM gives similar results that LASIK provides but, CM is Non-surgical, non-permanent (you can change the result if you need to), comfortable, available to all ages and FDA approved. The following slide shows the difference between the corneas of a patient who had LASIK versus his child who participates in Corneal Molding. The initial topographies (surface curvatures of the cornea) show a typical appearance.
You have to mold every night (OK, some patients with lower prescriptions can skip nights but that is the exception and not the rule). CM is not for firemen who have unpredictable sleep hours. It will not ‘fix a blind eye’. It is not proper for all prescriptions. All of this is linked to #1 as well.
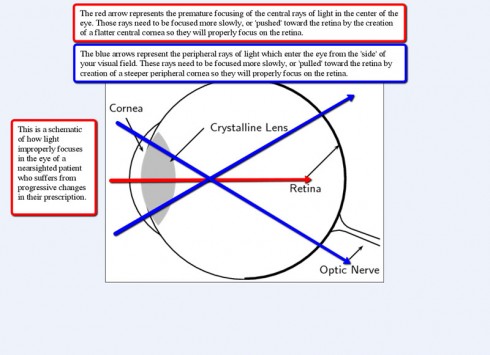
The results from LASIK and CM look very similar. Since these were both nearsighted patients before their procedures, the intended and realized topography change was to make the central part of the cornea flatter, which causes a ring of adjacent steepening (the red ring). This is important to understand. The nearsighted eye is too long (or has too strong of a corneal curvature). In order to see well the light entering the eye needs to be made more divergent (slow down the rate or speed of focusing or PUSHES THE FOCUS BACKWARD). This is done by making the curvature flatter or less sharply curved. The result of the central flattening is similar to any balanced math equation; the area next to the flattening must become steeper. That is the ‘red ring’ you see on both of these corneas. The ‘magic’ of the red ring is that steeper area focuses light more quickly or PULLS THE FOCUS FORWARD.
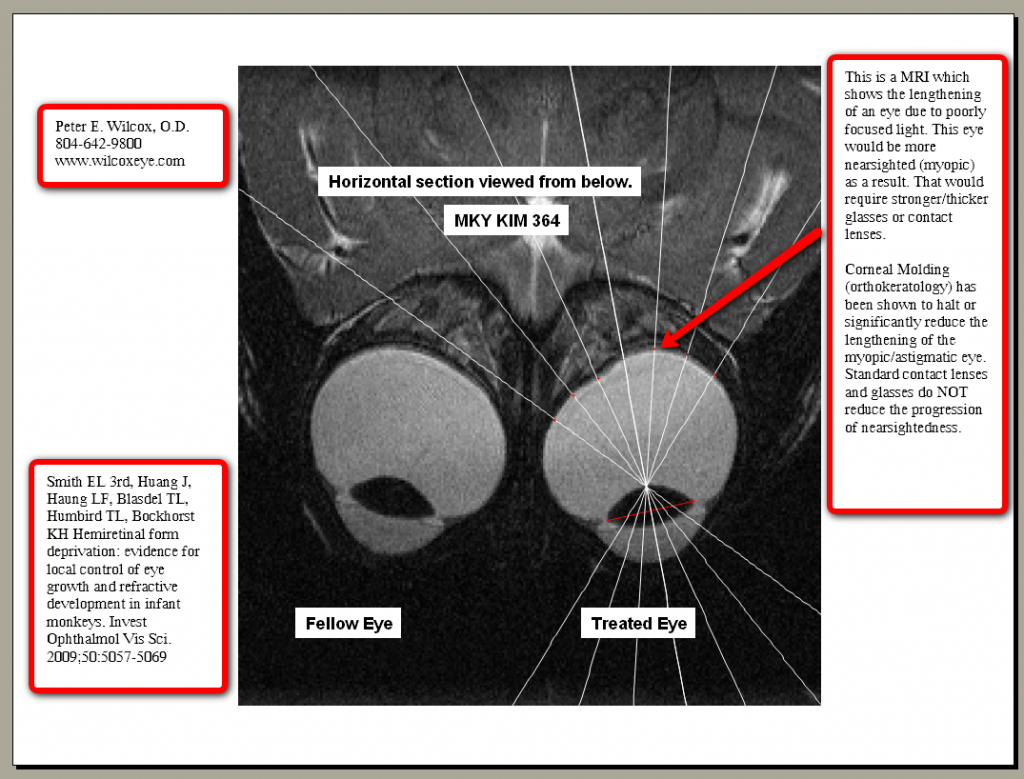
The result of this “pushing and pulling” of the light in the eye creates focused light in the whole back of the eye (“pan-retinal focus”). This is why and how the ‘kid who gets more nearsighted every year’ significantly slows to STOPS PROGRESSING! This is the most powerful tool we have to stabilize the younger eye.
There are other tools and procedures to slow the rate of progression of nearsightedness in the younger eye. Some are:
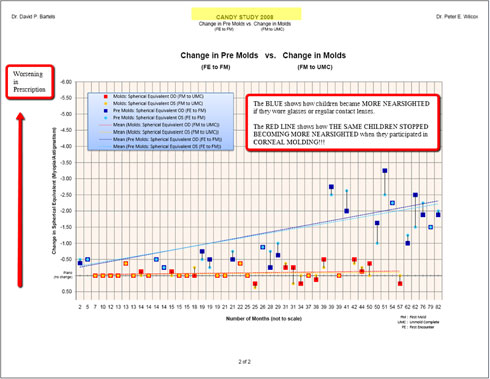
The CANDY Study (Controlling Astigmatism and Nearsightedness in Developing Youth) is a interoffice study performed by Dr. Wilcox and Dr. David Bartels (from New York) which showed that kids who participated in CM had a near total cessation in the progression of the nearsightedness which they were experiencing before CM. The graph below shows how the kids were getting worse before CM by an average of 0.50 diopters per year (blue line) and then only progressed at a near-zero rate of 0.05 diopters per year after starting CM (orange line). You can read the whole study here (CANDY Study, 2008).
Hyperopic Corneal Molding
Whereas very few doctors offer Corneal Molding (Orthokeratology) to their nearsighted patients, the molding of eyes for the correction of farsightedness reflects a fraction of those providers. The molding of a nearsighted eye requires a flattening to occur. The molding of a farsighted eye requires the opposite. The cornea must be made steeper after the lens is removed. This is much more difficult to accomplish. Dr. Wilcox successfully provides these results and assists in educating doctors so they may provide this to their patients.
Who is a candidate?
Farsighted patients of all ages.
Presbyopic patients in the need of reading glasses.
What are the limitations?
Though nearsighted patients with prescriptions as high as -10.00DS have been successfully molded by Dr. Wilcox and others, the ability to steepen a cornea is more difficult and the bar is much lower. To date Dr. Wilcox has alleviated +3.25DS in a 10 year old. The baseline topography and many other conditions are considered when forecasting success. It is safe to say that limits below +5.00 can be considered on a case-by-case basis.
Who is the typical patient?
Believe it or not, the patients who most utilize hyperopic molding are those with no distance prescription or are low hyperopes (farsighted) and over 40 years of age who need reading glasses and find them inconvenient. The hyperopic molded cornea is a center-near bifocal. These lens designs are routinely fit in soft and gas perm materials for all-day use. The molded result gives the patient daytime freedom from glasses and reading glasses. In some cases for those with higher distance prescriptions and stronger bifocal powers there can be a forecasted expectation that the patient may need a slight reading glass correction. That infrequently realized compromise is happily accepted by that population of patients who are otherwise crippled without their thick bifocal glasses.
If you can keep nearsighted kids from getting worse then why not have farsighted kids grow out of their refractive error?
Looking back at the young nearsighted molded eye reveals that the cessation (or significant slowing) of the eye’s axial length occurs due to the pulling the peripheral rays of light from their “retro-orbital focus” to a proper retinal or pre-retinal focus. The logic being exercised by a few of us in the world is a farsighted eye can be lengthened by pushing the peripheral light rays behind the eye. This is practiced by a few patients the WEC. At the worst, the farsighted child is glasses and contact lenses free all day. The huge bonus would be an increase in the axial length of the eye and a resultant out-growing of the patient’s hyperopia.
The reason to speak in the future tense is that this logic is simply that new. It will take time to see if these patients become less hyperopic. To achieve this conclusion we have sent our patients to a cataract surgeon for axial length measurements prior to their hyperopic molding. Annual refractive error and axial length measurements will determine if this cutting edge logic will be a reality. Low expectations and high hopes were discussed with the patient and parent. We will keep you posted in early summer 2013!!
It is the mission of the Wilcox Eye Center to exceed each patient’s expectations by providing the most comprehensive and highest quality vision care services and products available.
We will deliver this optimal level of eye care by remaining on the cutting edge through active research and continued education while investing in proven state-of-the-art technology.
We will treat each patient with respect and create an enduring relationship based on trust and honest communication.